
Original Investigation
Adjunctive Antipsychotics in Major Depressive Disorder. A Systematic Review and Network Meta-Analysis
Roger S. McIntyre, MD1,2,3; Stephen M. Stahl, MD, PhD4; Sung Ryul Shim, MPH, PhD5, et al. JAMA Psychiatry. Published Online: May 6, 2026. doi: 10.1001/jamapsychiatry.2026.0658
Key Points
Question How do US Food and Drug Administration (FDA)–approved atypical antipsychotics in major depressive disorder (MDD) compare with respect to overall efficacy and acceptability?
Findings In this systematic review and network meta-analysis, a hierarchy of efficacy and acceptability was observed, in which lumateperone had the highest effect size for efficacy, followed by aripiprazole, and in which aripiprazole had the highest overall acceptability, followed by cariprazine. Secondary and exploratory outcomes accorded with the coprimary outcomes across measures of efficacy, acceptability, and tolerability.
Meaning FDA-approved atypical antipsychotic agents for MDD exhibit differential efficacy, acceptability, and tolerability relevant to treatment selection and sequencing.
Abstract
Importance Most adults living with major depressive disorder (MDD) fail to achieve remission with conventional antidepressants. The US Food and Drug Administration (FDA) has approved 5 atypical antipsychotics in MDD on the basis of their substantial evidence of efficacy and safety.
Objective To compare the efficacy and acceptability of FDA-approved atypical antipsychotics for the adjunctive treatment of MDD in order to provide decision support to practitioners and persons with lived experience.
Data Sources A systematic search was conducted using PubMed/MEDLINE, PsycINFO, the Cochrane Library, and Embase from database inception through July 15, 2025.
Study Selection Six independent raters screened publications for eligibility. Inclusion criteria were atypical antipsychotics that are FDA approved in the adjunctive treatment of MDD.
Data Extraction and Synthesis Two independent raters obtained data and examined risk of bias in accordance with the Cochrane criteria. Effect sizes were synthesized using random-effects models. Data were analyzed from August to September 2025.
Main Outcomes and Measures The primary outcomes were efficacy (ie, ≥50% reduction from baseline in the total Montgomery-Åsberg Depression Rating Scale [MADRS] score) and acceptability (ie, all-cause discontinuation).
Results A total of 22 short-term studies comprising 10 962 participants (aripiprazole: n = 1297; brexpiprazole: n = 1973; cariprazine: n = 1894; lumateperone: n = 483; quetiapine extended release [XR]: n = 719; and placebo: n = 4596) were included for analysis. Lumateperone had the highest effect size for efficacy (risk ratio [RR], 1.72; 95% credible interval [CrI], 1.40-2.15), followed by aripiprazole (RR, 1.53; 95% CrI, 1.32-1.77), brexpiprazole (RR, 1.38; 95% CrI, 1.18-1.65), cariprazine (RR, 1.20; 95% CrI, 1.07-1.36), and quetiapine XR (RR, 1.15; 95% CrI, 0.96-1.35). A hierarchy of acceptability was observed, with aripiprazole exhibiting the highest acceptability (RR, 1.16; 95% CrI, 0.89-1.50), followed by cariprazine (RR, 1.44; 95% CrI, 1.15-1.82), brexpiprazole (RR, 1.47; 95% CrI, 1.18-1.85), quetiapine XR (RR, 1.56; 95% CrI, 1.14-2.12), and lumateperone (RR, 2.30; 95% CrI, 1.45-3.84). Secondary outcomes (eg, symptomatic remission) and exploratory outcomes (eg, clinically significant weight gain) accorded with the coprimary outcomes.
Conclusions and Relevance This systematic review and meta-analysis indicates that differences exist between adjunctive atypical antipsychotics in the treatment of MDD with respect to overall efficacy and acceptability, which should be simultaneously considered. The absence of adequate and well-controlled studies documenting maintenance efficacy of adjunctive atypical antipsychotics in MDD remains a knowledge gap.
Introduction
It has long been accepted that a substantial percentage of adults living with major depressive disorder (MDD) prescribed and self-administered antidepressants inadequately benefit, as evidenced by persisting depressive symptoms and deficits across patient-reported outcomes (eg, health-related quality of life, positive mental health, overall function).1–4 The hazards of nonremission are well documented and include, but are not limited to, higher rates of recurrence, chronicity of illness, incidence of medical and psychiatric comorbidity, suicidality, health care service utilization and health-related costs, as well as patient frustration and dissatisfaction with treatment.1,5
Although combining antidepressants is not uncommon practice, the adjunctive combination of select atypical antipsychotics in MDD has been US Food and Drug Administration (FDA) approved and/or is supported by a replicated evidence base of adequate and well-controlled short-term studies.6 For example, aripiprazole, brexpiprazole, cariprazine, lumateperone, and quetiapine extended release (XR) are all FDA-approved adjunctive therapies for the treatment of adults with MDD exhibiting inadequate response to antidepressants. In addition, the fixed-dose combination formulation olanzapine-fluoxetine is established as efficacious in adults with treatment-resistant depression (TRD).7
Whether differences exist between the FDA-approved atypical antipsychotics in MDD with respect to overall efficacy and acceptability is currently unknown and is highly relevant to shared decision-making. For example, it is well established that significant differences exist between atypical antipsychotics with respect to certain tolerability aspects that predispose treatment discontinuation (eg, psychotropic drug–related weight gain, drug-induced movement disorders).8,9
Herein, we conducted a systematic review and network meta-analysis of all currently FDA-approved adjunctive atypical antipsychotics in adults with MDD. Studies reporting on the efficacy of atypical antipsychotic monotherapy in MDD were not included, as this approach is not clinically recommended in most jurisdictions.10–12 Studies pertaining to antidepressant combinations or select atypicals that are not FDA-approved in MDD (eg, risperidone) were also not included, as they do not have substantial evidence of efficacy as defined by 2 adequate, positive, pivotal, well-controlled, double-blind, placebo-controlled randomized clinical trials (RCTs). Furthermore, olanzapine-fluoxetine was excluded from the analysis, as the emphasis was on atypical antipsychotics evaluated and FDA-approved in MDD in adults who were inadequate responders rather than those meeting criteria for TRD.1,13 It is the view of the FDA that the nomenclature pertaining to adequacy of response in MDD and TRD is imprecise and undoubtedly includes overlapping populations.1
Methods
Identification and Selection of Studies
Search Strategy
The study protocol was registered on PROSPERO (CRD420251114117). A systematic search was conducted using the databases PubMed/MEDLINE, PsycINFO, the Cochrane Library, and Embase using medical subject heading terms and text keywords. All relevant studies were also manually searched from the US National Institutes of Health–funded clinical trial registry, the European Union clinical trial registry, and Google Scholar. The searches were conducted from database inception through July 15, 2025, and no language restrictions were imposed. The 2 lumateperone studies that were identified and included were not published at the time of the analysis; access to these studies was provided by the first author, who is a coauthor on one of the studies (ie, study 501),14and the sponsor, Intra-Cellular Therapies, provided a copy of the second study (ie, study 502)15on request for the purpose of the network analysis. Both studies were subsequently published in 2025. Additional details are listed in the eMethods in Supplement 1 (eTables 1-3 in Supplement 1).
Eligibility Criteria
Inclusion criteria were established prior to article reviews and were as follow: (1) patients aged 18 years or older with a diagnosis of MDD using standardized diagnostic criteria (eg, DSM-IV, DSM-IV-TR, DSM-5, and DSM-5-TR) with inadequate responses to previous antidepressant trials; and (2) double-blind pivotal RCTs comparing FDA-approved adjunctive atypical antipsychotic therapies (ie, antidepressants combined with either aripiprazole, brexpiprazole, cariprazine, quetiapine XR, or lumateperone) to placebo.
Main Outcomes and Measures
The main outcomes were efficacy (ie, response defined as ≥50% improvement in overall depressive symptom severity using the Montgomery-Åsberg Depression Rating Scale [MADRS]) and acceptability (ie, all-cause discontinuation rate). The secondary outcome measures included remission (MADRS total score ≤8 or ≤10), change in overall severity of depressive symptoms, and discontinuation due to adverse events.
The outcome measures for efficacy, remission, and severity of depressive symptoms were based on the MADRS score, and the primary end point was at week 6, which accords with regulatory guidance in evaluating acute adjunctive efficacy in MDD.16Definitions of all outcome measures are listed in eTable 3 in Supplement 1. In addition to the aforementioned outcome measures, the following exploratory outcomes were also examined: Clinical Global Impressions–Severity (CGI-S), CGI-Improvement (CGI-I), 7% or greater weight gain, Sheehan Disability Scale (SDS), and extrapyramidal symptoms.17 ,18 Information on data extraction and quality assessment is listed in the eMethods in Supplement 1.
Statistical Analysis
First, we estimated a mean difference (MD) for a continuous outcome (standardized mean difference was not used as all studies used the MADRS as the primary efficacy parameter), severity of depressive symptoms, and risk ratios (RRs) for all other dichotomous outcomes and their corresponding 95% credible intervals ([CrIs] for bayesian approach) and 95% confidence intervals (for frequentist approach) using network meta-analyses. A single study identified that limited enrollment to the geriatric population (ie, age ≥60 years) was excluded from the main analysis due to potential heterogeneity.19 The geriatric study was, however, included in the sensitivity analysis.19
Group-level data and the normal likelihood function were used for continuous outcomes, and the binomial likelihood function was used for dichotomous outcomes. The study effect sizes were then synthesized using random-effects models. In particular, the gemtc package in R software version 4.3.1 (R Foundation for Statistical Computing) was used for bayesian network meta-analysis.20 ,21 Additional details (eg, bayesian and frequentist estimates) are provided in the eMethods in Supplement 1.
After conducting the main analyses, multiple subgroup and sensitivity analyses were also conducted using both bayesian and frequentist approaches. The analyses were repeated (1) with the inclusion of the study that had the older adult population only; (2) with studies published in or after 2010 only (to attenuate the placebo effects over time); and (3) stratified by individual dose (to understand dose-specific treatment effects better; see eTable 4 in Supplement 1 for rationale).19 Unless otherwise noted, a 2-sided P value less than .05 was considered statistically significant.
Results
Study Selection Process
The literature search yielded 1407 articles, of which 65 were eligible after screening titles and abstracts and removing duplicates. Of the eligible studies, 45 were further excluded after full-text screening. Six independent investigators (R.S.M., S.R.S., A.T.H.K., C.E.D., H.X., and T.G.R.) discovered 6 additional studies by manually searching reference lists, clinical registries, and Google Scholar, and 2 of these studies were included (eFigure 1 in Supplement 1).
Study Characteristics
A total of 22 studies comprising 10 962 participants (n = 1297 patients receiving aripiprazole; n = 1973 patients receiving brexpiprazole; n = 1894 patients receiving cariprazine; n = 483 patients receiving lumateperone; n = 719 patients receiving quetiapine XR; and n = 4596 patients receiving placebo) were included in the systematic review and network meta-analyses (eTable 3 in Supplement 1).19 ,22–42 All of the included RCTs were double blind and conducted in the outpatient setting, and 21 of 22 RCTs (95.5%) had sponsorship from industry (eTable 3 in Supplement 1). eTable 3 in Supplement 1 provides details of study characteristics, including mean age, proportion of female sex, and dosing information for all included studies. Meta-analytical networks were formulated (Figure 1).
Figure 1. Network Plot of Primary Outcomes, Efficacy and Acceptability
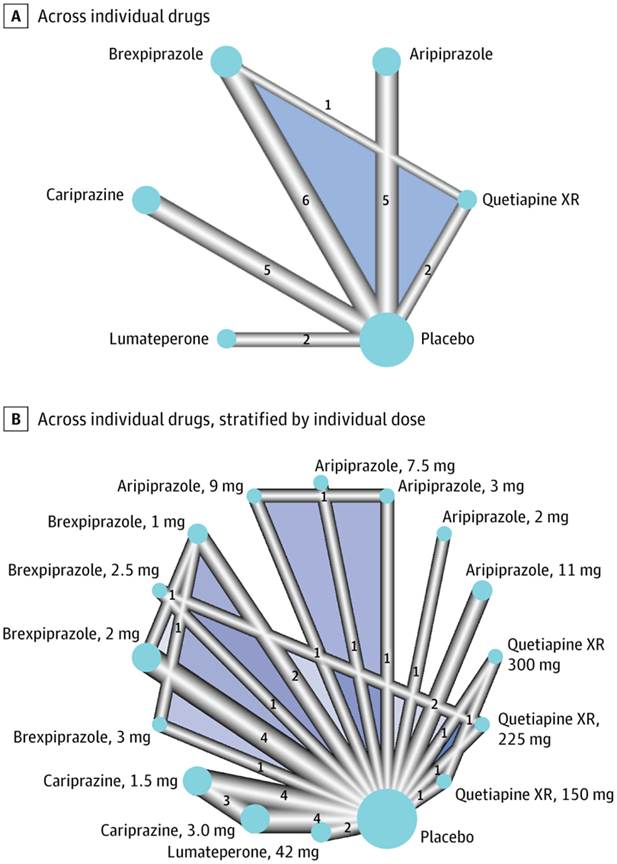
Across individual drugs (A) and stratified by individual drugs (B). The lines link treatments that were directly compared in randomized clinical trials (RCTs). The thickness of the lines corresponds to the number of RCTs evaluating the comparison. The size of the nodes corresponds to the number of participants assigned to the treatment. XR indicates extended release.
Primary Outcomes: Efficacy and Acceptability
Compared to placebo, lumateperone had the highest efficacy (RR, 1.72; 95% CrI, 1.40-2.15), followed by aripiprazole (RR, 1.53; 95% CrI, 1.32-1.77), brexpiprazole (RR, 1.38; 95% CrI, 1.18-1.65), cariprazine (RR, 1.20; 95% CrI, 1.07-1.36), and quetiapine XR (RR, 1.15; 95% CrI, 0.96-1.35) (Figure 2A).
Figure 2. Forest Plots Showing Efficacy (Response Rate [A]) and Acceptability (Dropout Rate [B]) at the End of Treatment (Week 6)
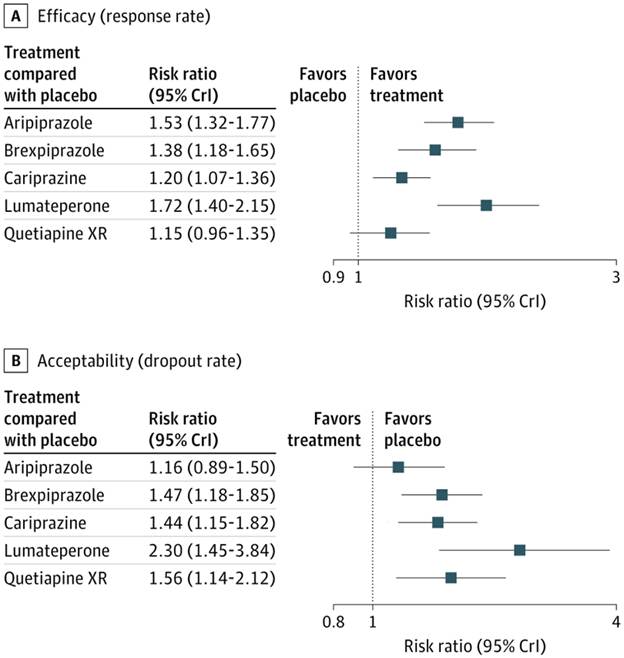
XR indicates extended release.
The highest acceptability was noted for aripiprazole (RR, 1.16; 95% CrI, 0.89-1.50), followed hierarchically by cariprazine (RR, 1.44; 95% CrI, 1.15-1.82), brexpiprazole (RR, 1.47; 95% CrI, 1.18-1.85), quetiapine XR (RR, 1.56; 95% CrI, 1.14-2.12), and lumateperone (RR, 2.30; 95% CrI, 1.45-3.84) compared to placebo (Figure 2B).
Surface under the cumulative ranking curve (SUCRA) values also aligned with the aforementioned hierarchy of efficacy and acceptability (eFigure 2 in Supplement 1). Pairwise comparisons of individual drugs are listed in the league table (eTable 5 in Supplement 1). These findings are consistent in the frequentist approach (eFigures 3 and 4 in Supplement 1) and in the following subgroup analyses: (1) network meta-analyses with the inclusion of the older adult population (eFigures 5-8 in Supplement 1) and (2) network meta-analyses with studies published in or after 2010 (eFigures 9-12 in Supplement 1).
Primary Outcomes: Efficacy and Acceptability, Stratified by Individual Dose
When compared to placebo, lumateperone, 42 mg, had the greatest effect size for efficacy (RR, 1.73; 95% CrI, 1.42-2.16), followed by aripiprazole, 11 mg (RR, 1.67; 95% CrI, 1.36-2.04), and aripiprazole, 3 mg (RR, 1.49; 95% CrI, 1.09-2.03) (Figure 3A). For acceptability, however, lumateperone, 42 mg, had overall lower estimate compared to placebo (RR, 2.35; 95% CrI, 1.49-3.81), followed by quetiapine XR, 300 mg (RR, 1.80; 95% CrI, 1.25-2.68), and brexpiprazole, 2 mg (RR, 1.63; 95% CrI, 1.24-2.16) (Figure 3B). SUCRA values showed similar patterns (eFigure 13 in Supplement 1). These findings were consistent in the frequentist approach (eFigures 14 and 15 in Supplement 1) and in the following subgroup analyses: (1) network meta-analyses with the inclusion of the older adult population (eFigures 16-19 in Supplement 1) and (2) network meta-analyses with studies published in or after 2010 (eFigures 20-23 in Supplement 1).
Figure 3. Forest Plots of Adjunctive Antipsychotics vs Placebo for Primary Outcomes, Stratified by Individual Dose, at the End of Treatment (Week 6)
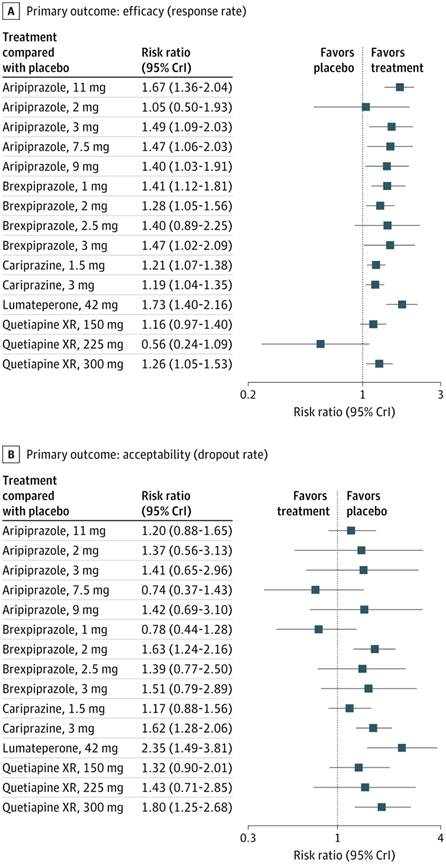
Panels represent primary outcomes of efficacy (response [A]) and acceptability (dropout rate [B]). Network meta-analytic estimates of treatment effect of each drug vs placebo are reported as risk ratios (RRs) or mean differences and their corresponding 95% credible intervals (CrIs). For efficacy, an RR >1.0 favors the treatment compared to placebo. For acceptability, an RR <1.0 favors the treatment compared to placebo. XR indicates extended release.
Secondary Outcomes: Remission, Severity of Depressive Symptoms, and Discontinuation Due to Adverse Events
Lumateperone, when compared to placebo, had the greatest effect size for remission (RR, 1.87; 95% CrI, 1.31-2.69) and reduction in overall severity of depressive symptoms (MD, −4.83; 95% CrI, −6.42 to −3.21), followed by aripiprazole (RR, 1.58; 95% CrI, 1.28-1.95; MD, −2.34; 95% CrI, −3.33 to −1.37) (Figure 4).
Figure 4. Forest Plots Showing Secondary Outcomes at the End of Treatment (Week 6)
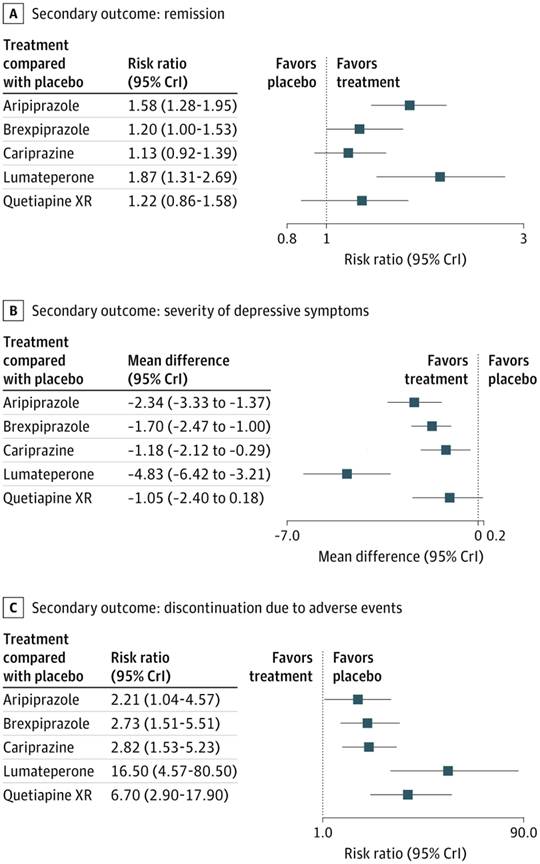
Panels represent secondary outcomes of remission (A), severity of depressive symptoms (B), and discontinuation due to adverse events (C). Network meta-analytic estimates of treatment effect of each drug versus placebo are reported as risk ratios (RRs) or mean differences and their corresponding 95% credible intervals (CrIs). For efficacy and remission, a risk ratio (RR) >1.0 favors the treatment compared to placebo. For severity of depressive symptoms, a mean difference <0 favors the treatment compared to placebo. For acceptability and discontinuation due to adverse events, an RR <1.0 favors the treatment compared to placebo. XR indicates extended release.
For discontinuation due to adverse events, lumateperone had a relatively higher rate (RR, 16.50; 95% CrI, 4.57-80.50), followed by quetiapine XR (RR, 6.70; 95% CrI, 2.90-17.90) (Figure 4). These results were consistent with SUCRA values. Findings were similar in the frequentist approach (eFigures 3 and 4 in Supplement 1) and in the following subgroup analyses: (1) network meta-analyses with the inclusion of the older adult population (eFigures 5-8 in Supplement 1) and (2) network meta-analyses with studies published in or after 2010 (eFigures 9-12 in Supplement 1). Pairwise comparisons of individual drugs are listed in the league table (eTable 5 in Supplement 1).
Secondary Outcomes: Remission, Severity of Depressive Symptoms, and Discontinuation Due to Adverse Avents, Stratified by Individual Dose
Lumateperone, 42 mg, compared to placebo had the greatest effect size for remission (RR, 1.86; 95% CrI, 1.33-2.62), followed by aripiprazole, 11 mg (RR, 1.77; 95% CrI, 1.35-2.36) (Figure 5A), and for reduction in severity of depressive symptoms (lumateperone, 42 mg: MD, −4.85; 95% CrI, −6.54 to −3.15; aripiprazole, 11 mg: MD, −3.27; 95% CrI, −5.07 to −1.45) (Figure 5B).
Figure 5. Forest Plots Showing Secondary Outcomes at the End of Treatment, Stratified by Individual Dose (at the End of Treatment [Week 6])
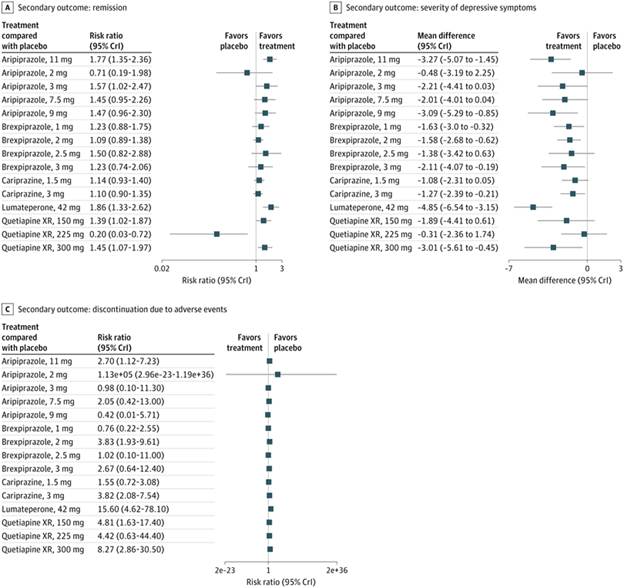
Panels represent secondary outcomes of remission (A), severity of depressive symptoms (B), and discontinuation due to adverse events (C). Network meta-analytic estimates of treatment effect of each drug vs placebo are reported as risk ratios (RRs) or mean differences and their corresponding 95% credible intervals (CrIs). For efficacy and remission, an RR >1.0 favors the treatment compared to placebo. For severity of depressive symptoms, a mean difference <0 favors the treatment compared to placebo. For acceptability and discontinuation due to adverse events, an RR <1.0 favors the treatment compared to placebo. XR indicates extended release.
For discontinuation due to adverse events, lumateperone, 42 mg, had the highest rate (RR, 15.60; 95% CrI, 4.62-78.10), followed by quetiapine XR, 300 mg (RR, 8.27; 95% CrI, 2.86-30.50) (Figure 5C). Findings of SUCRA estimates are consistent with these findings (eFigure 13 in Supplement 1). These main findings are consistent in the frequentist approach (eFigures 14 and 15 in Supplement 1) and in the following subgroup analyses: (1) network meta-analyses with the inclusion of the older adult population (eFigures 16-19 in Supplement 1) and (2) network meta-analyses with studies published in or after 2010 (eFigures 20-23 in Supplement 1). Pairwise comparisons of individual drugs stratified by individual dose are listed in the league table (eTable 6 in Supplement 1).
Exploratory Outcomes
For overall extrapyramidal symptoms, tremor and/or akathisia individual drugs were not significantly different from placebo (eFigure 24 in Supplement 1). Similar patterns were found when stratified by the individual dose (eFigure 25 in Supplement 1).
Model Assumptions and Publication Bias
We used the node-splitting method, which showed consistency between direct and indirect comparisons for all individual outcomes (all nonsignificant); no evidence of inconsistency was detected. In our primary analyses, we did not find any publication bias using the funnel plots, Egger tests, and Begg and Mazumdar tests (eFigure 26 in Supplement 1) and in subgroup analyses with the inclusion of older adult populations and analyses using publications in or after 2010 (eFigures 27 and 28 in Supplement 1). We also did not detect any potential publication bias in all network meta-analyses stratified by individual dose (eFigures 29-31 in Supplement 1).
Risk of Bias and Justification
Methodological quality of the included studies was rated low to high; justification is provided in eTable 7 in Supplement 1. Overall, 4 of 22 studies (18.2%) had some concerns for bias, and the other 18 of 22 studies (81.8%) had a low risk of bias.
Discussion
Taken together, these results indicate that the magnitude of improvement in depressive symptoms observed with adjunctive atypical antipsychotics is clinically meaningful (ie, ≥2 point improvement as measured by the MADRS compared to placebo).43–45 In addition, a hierarchy of efficacy (ie, response rate) was observed across the agents, with lumateperone followed by aripiprazole exhibiting higher relative efficacy. The relatively higher efficacy estimate for lumateperone was also supported by the secondary outcomes (eg, remission, overall depressive symptom improvement), as well as exploratory efficacy measures (eg, improvement in overall CGI-S and CGI-I scores and/or SDS).
A hierarchy of acceptability (ie, all-cause discontinuation rate) was also observed, with dopamine partial agonists (eg, aripiprazole, cariprazine, brexpiprazole) at the higher end of acceptability and quetiapine XR and lumateperone at the lower end. Results from the secondary outcome measures (ie, discontinuation due to adverse events) accorded with the coprimary outcomes. Also, results from the exploratory outcomes were largely supportive of the coprimary and secondary outcomes. Some of the exploratory outcomes, however, were discordant with the primary and secondary outcomes (eg, lumateperone was the only atypical antipsychotic not associated with a ≥7% weight increase compared to placebo, despite having lower overall acceptability) (eFigures 24 and 25 in Supplement 1).8,46
The acceptability of atypical antipsychotics is influenced by dosing initiation, titration, and target dosing. For example, aripiprazole, brexpiprazole, cariprazine, and quetiapine XR were studied using multiple fixed-dose and flexible-dose paradigms, while lumateperone was evaluated with a single fixed-dose design (ie, 42 mg). Whether initiating lumateperone at a lower dose (ie, 10.5 mg or 21 mg) and titrating to 42 mg as the target dose and/or implementing a flexible-dose design would have affected overall acceptability remains an open question.11 Dosing initiation, titration, and flexibility may inadvertently conflate tolerability with study design, which should be considered when interpreting our results.
Limitations
There are methodological aspects to our analysis that limit inferences and interpretations of our findings. First, most studies were industry sponsored with 1 exception (Lenze and colleagues,19 2015), and there are no head-to-head trials comparing atypical antipsychotics in the treatment of adults with MDD. In addition, eligibility was confined to those studies that enrolled adults aged 18 years or older, and results cannot be generalized to the pediatric population.47,48 This systematic review and network meta-analysis only included studies evaluating the short-term efficacy, tolerability, and safety of select adjunctive atypical antipsychotic agents in MDD that have been FDA-approved and supported by large, replicated pivotal trials.49
These results also need to be interpreted cautiously, as heterogeneity in the sample composition enrolled in each of the component studies could significantly affect the hierarchy of efficacy and/or tolerability observed. For example, differences in the baseline depression severity and duration of the index depressive episode, as well as the treatment history, could meaningfully affect not only the efficacy estimate of the atypical antipsychotic, but also response to placebo and drug-placebo difference. Hence, differences observed across atypical agents may not fully reflect intrinsic differences in pharmacology but instead may be by-products of the aforementioned sample heterogeneity.
Furthermore, we did not endeavor to identify baseline sociodemographic or illness characteristics that may moderate treatment outcomes for each of the atypical antipsychotics. For example, depressive episodes are highly heterogeneous, and clinicians often select an atypical antipsychotic to target specific phenomenological features.11,50–69 It should not be assumed that the efficacy hierarchy that we have observed, obtained in heterogeneous populations, would reflect the efficacy of each atypical antipsychotic in specifically targeting phenomenological features, such as mixed features, anxious distress, anhedonia, and rumination. Also, a cost-effectiveness analysis was not conducted, and concealment of allocation was not evaluated in the included studies.
The definition of inadequate response was not identical across the 5 atypical antipsychotic agents analyzed herein. For example, the studies that evaluated aripiprazole and brexpiprazole defined inadequate response as historical failure to 1 to 3 prior antidepressants, as well as a prospective antidepressant failure (ie, brexpiprazole). Studies evaluating cariprazine and lumateperone defined inadequate response as historical failure to 1 to 2 prior antidepressants without the requirement for a prospective antidepressant failure. With respect to quetiapine XR, the number of prior antidepressants and inadequate response was not consistently specified.
The magnitude of improvement in participants assigned to placebo influences the effect size estimates of the active treatment. As with all clinical trial programs, the placebo response in persons with MDD in the trials that we included were highly variable. For example, the overall improvement in the MADRS total score at week 6 in persons assigned to placebo were as follows: aripiprazole, −5.8 to −6.4; brexpiprazole, −5.15 to −6.33; cariprazine, −11.5 to −12.5; quetiapine XR, −11.7 to 12.21; and lumateperone, −9.8 to −10.2. Hence, a hierarchy of placebo response was also observed, with the highest placebo response in the cariprazine trials and lowest placebo response in the aripiprazole and brexpiprazole studies. Consequently, the positioning of each agent in the estimated efficacy hierarchy needs to be carefully interpreted within the broader context of meaningful differences across the studies in the placebo response.
Priority research vistas are the need for acute and/or long-term head-to-head comparative effectiveness studies in MDD comparing atypical antipsychotics to each other as well as alternative antidepressant switch options (eg, bupropion combination) or neuromodulation.70–75 Whether the 5 atypical antipsychotics herein are efficacious in adults with TRD and their relative efficacy to intranasal esketamine are additional priority research questions.70,76–80
Conclusions
Overall, this systematic review and network meta-analysis indicates that efficacy and acceptability differences exist between adjunctive atypical antipsychotics in the treatment of adults with MDD in inadequate response to antidepressants. Clinical decisions regarding atypical antipsychotics need to simultaneously weigh estimated relative efficacy as well as acceptability. These results address an important knowledge gap and provide decision support to practitioners and persons with lived experience, as well as providing data to inform treatment algorithms, policy, and reimbursement considerations.
Although this study focused on FDA-approved agents, not all agents are approved in other jurisdictions (ie, quetiapine XR is the only agent approved by the European Medicine Agencies in MDD). The absence of long-term maintenance efficacy for any adjunctive atypical antipsychotic remains a knowledge gap (although monotherapy maintenance therapy exists for quetiapine XR) and has precluded approvals of many atypicals in some jurisdiction in MDD (eg, European Medicine Agencies).81,82
Article Information
Accepted for Publication: February 10, 2026.
Published Online: May 6, 2026. doi:10.1001/jamapsychiatry.2026.0658
Corresponding Author: Roger S. McIntrye, MD, Brain and Cognition Discovery Foundation, 77 Bloor St W, Ste 617, Toronto, ON M5S 1M2, Canada (roger.mcintyre@bcdf.org)
Author Contributions: Dr McIntyre had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: McIntyre, Stahl, Shim, Goldberg, Correll, Kwan, Rhee.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: McIntyre, Shim, Kwan, Rhee.
Critical review of the manuscript for important intellectual content: All authors.
Statistical analysis: Shim, Goldberg, Rhee.
Administrative, technical, or material support: McIntyre, Stahl, Shim, Kwan, Dri, Rhee.
Supervision: McIntyre, Correll, Rhee.
Conflict of Interest Disclosures: Dr McIntyre reported grants from the Canadian Institutes of Health Research, the Global Alliance for Chronic Diseases, the Milken Institute, and the National Natural Science Foundation of China and speaker or consultation fees from AbbVie, Alkermes, atai Life Sciences, Axsome Therapeutics, Bausch Health, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Eisai, Intra-Cellular Therapies, Janssen, Kris, Lundbeck, the Milken Institute, Mitsubishi Tanabe, Neumora Therapeutics, NeuraWell Therapeutics, Neurocrine Biosciences, NewBridge Pharmaceuticals, Novo Nordisk, Otsuka, Pfizer, Purdue, Sage, Sanofi, Sunovion, Takeda, and Viatris outside the submitted work. Dr Stahl reported personal fees from AbbVie, Acadia, AdhereTech, Alkermes, Autobahn, Axsome Therapeutics, Aytu BioPharma, Bristol Myers Squibb, Clexio Biosciences, Delix Therapeutics, Intra-Cellular Therapies, LivaNova, Lundbeck, Neurocrine Biosciences, Otsuka, Supernus Pharmaceuticals, Tonix Pharmaceuticals, and Vanda Pharmaceuticals during the conduct of the study and stock options in Delix Therapeutics, Genomind, Lipidio Pharmaceuticals, and NeuraWell Therapeutics. Dr Pompili reported receiving lecture and advisory board honoraria or engaged in clinical trial activities in the last 5 years with AbbVie, Angelini Pharma, Boehringer Ingelheim, EG Stada, Fidia, Johnson & Johnson, Lundbeck, Merck Sharp & Dohme, Newron Pharmaceuticals, Neopharmed Gentili, Otsuka, Pfizer, Recordati, Rovi, Teva, and Viatris outside the submitted work. Dr Goldberg reported personal fees from AbbVie, Alkermes, Alvogen, Axsome Therapeutics, Bristol Myers Squibb, Intra-Cellular Therapies, Johnson & Johnson, Otsuka, and Vanda Pharmaceuticals and royalties from American Psychiatric Publishing and from Cambridge University Press outside the submitted work. Dr Correll reported royalties fees from UpToDate; serving as a consultant and/or advisor to or receiving honoraria from AbbVie, Alkermes, Allergan, Angelini, Aristo, Boehringer Ingelheim, Bristol Myers Squibb, Cardio Diagnostics, Cerevel, CNX Therapeutics, Compass Pathways, Darnitsa, Delpor, Denovo, Eli Lilly, Gedeon Richter, Hikma, Holmusk, Intra-Cellular Therapies, Jamjoom Pharma, Janssen/Johnson & Johnson, Karuna, LB Pharma, Lundbeck, MapLight Therapeutics, MedinCell, MedLink, Merck, Mindpax, Mitsubishi Tanabe Pharma, Mylan, Neumora Therapeutics, Neurocrine Biosciences, Neurelis, Newron, Noven, Novo Nordisk, Otsuka, PPD Biotech, Recordati, Relmada, Reviva, Rovi, Saladax, Sanofi, Seqirus, Servier, Sumitomo Pharma America, Sunovion, Sun Pharma, Supernus Pharmaceuticals, Tabuk, Takeda, Terran, Teva, Tolmar, Vertex, Viatris, and Xenon Pharmaceuticals; providing expert testimony for Janssen, Lundbeck, and Otsuka; serving on a data safety monitoring board for Compass Pathways, Intra-Cellular Therapies, Relmada, Reviva, and Rovi; receiving grants from Boehringer Ingelheim, Janssen, and Takeda; and having stock options in Cardio Diagnostics, Kuleon Biosciences, LB Pharma, Medlink, Mindpax, Quantic, and Terran outside the submitted work. Dr Vinberg reported speaker fees from Eli Lilly, Johnson & Johnson, and Lundbeck outside the submitted work. No other disclosures were reported.
Funding/Support: None reported.
Data Sharing Statement: See Supplement 2.
References
1.
McIntyre RS, Alsuwaidan M, Baune BT, et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. 2023;22(3):394-412. doi:10.1002/wps.21120PubMedGoogle ScholarCrossref
2.
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357-1366. doi:10.1016/S0140-6736(17)32802-7PubMedGoogle ScholarCrossref
3.
Rush AJ. STAR*D: what have we learned? Am J Psychiatry. 2007;164(2):201-204. doi:10.1176/ajp.2007.164.2.201PubMedGoogle ScholarCrossref
4.
Pigott HE, Kim T, Xu C, Kirsch I, Amsterdam J. What are the treatment remission, response and extent of improvement rates after up to four trials of antidepressant therapies in real-world depressed patients? a reanalysis of the STAR*D study’s patient-level data with fidelity to the original research protocol. BMJ Open. 2023;13(7):e063095. doi:10.1136/bmjopen-2022-063095PubMedGoogle ScholarCrossref
5.
Mago R, Fagiolini A, Weiller E, Weiss C. Understanding the emotions of patients with inadequate response to antidepressant treatments: results of an international online survey in patients with major depressive disorder. BMC Psychiatry. 2018;18(1):33. doi:10.1186/s12888-018-1625-yPubMedGoogle ScholarCrossref
6.
Henssler J, Alexander D, Schwarzer G, Bschor T, Baethge C. Combining antidepressants vs antidepressant monotherapy for treatment of patients with acute depression: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(4):300-312. doi:10.1001/jamapsychiatry.2021.4313
ArticlePubMedGoogle ScholarCrossref
7.
Thase ME, Corya SA, Osuntokun O, et al. A randomized, double-blind comparison of olanzapine/fluoxetine combination, olanzapine, and fluoxetine in treatment-resistant major depressive disorder. J Clin Psychiatry. 2007;68(2):224-236. doi:10.4088/JCP.v68n0207PubMedGoogle ScholarCrossref
8.
McIntyre RS, Kwan ATH, Rosenblat JD, Teopiz KM, Mansur RB. Psychotropic drug-related weight gain and its treatment. Am J Psychiatry. 2024;181(1):26-38. doi:10.1176/appi.ajp.20230922PubMedGoogle ScholarCrossref
9.
Siafis S, Wu H, Wang D, et al. Antipsychotic dose, dopamine D2 receptor occupancy and extrapyramidal side-effects: a systematic review and dose-response meta-analysis. Mol Psychiatry. 2023;28(8):3267-3277. doi:10.1038/s41380-023-02203-yPubMedGoogle ScholarCrossref
10.
Nishi A, Sawada K, Uchida H, Mimura M, Takeuchi H. Antipsychotic monotherapy for major depressive disorder: a systematic review and meta-analysis. Pharmacopsychiatry. 2023;56(1):5-17. doi:10.1055/a-1934-9856PubMedGoogle ScholarCrossref
11.
Durgam S, Kozauer SG, Earley WR, et al. Lumateperone for the treatment of major depressive disorder with mixed features or bipolar depression with mixed features: a randomized placebo-controlled trial. J Clin Psychopharmacol. 2025;45(2):67-75. doi:10.1097/JCP.0000000000001964PubMedGoogle ScholarCrossref
12.
Stahl SM, Morrissette DA, Faedda G, et al. Guidelines for the recognition and management of mixed depression. CNS Spectr. 2017;22(2):203-219. doi:10.1017/S1092852917000165PubMedGoogle ScholarCrossref
13.
Maj M, Stein DJ, Parker G, et al. The clinical characterization of the adult patient with depression aimed at personalization of management. World Psychiatry. 2020;19(3):269-293. doi:10.1002/wps.20771PubMedGoogle ScholarCrossref
14.
Durgam S, Earley WR, Kozauer SG, et al. Lumateperone as adjunctive therapy in patients with major depressive disorder: results from a randomized, double-blind, phase 3 trial. J Clin Psychiatry. 2025;86(4):25m15848. doi:10.4088/JCP.25m15848PubMedGoogle ScholarCrossref
15.
Durgam S, Earley WR, Kozauer SG, et al. Adjunctive lumateperone in patients with major depressive disorder: results from a randomized, double-blind, phase 3 trial. Am J Psychiatry. 2025;182(12):1072-1082. doi:10.1176/appi.ajp.20250292PubMedGoogle ScholarCrossref
16.
Center for Drug Evaluation, US Food & Drug Administration. Major depressive disorder: developing drugs for treatment. April 24, 2020. Accessed July 4, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/major-depressive-disorder-developing-drugs-treatment
17.
Leon AC, Olfson M, Portera L, Farber L, Sheehan DV. Assessing psychiatric impairment in primary care with the Sheehan Disability Scale. Int J Psychiatry Med. 1997;27(2):93-105. doi:10.2190/T8EM-C8YH-373N-1UWDPubMedGoogle ScholarCrossref
18.
Busner J, Targum SD. The Clinical Global Impressions Scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4(7):28-37.PubMedGoogle Scholar
19.
Lenze EJ, Mulsant BH, Blumberger DM, et al. Efficacy, safety, and tolerability of augmentation pharmacotherapy with aripiprazole for treatment-resistant depression in late life: a randomised, double-blind, placebo-controlled trial. Lancet. 2015;386(10011):2404-2412. doi:10.1016/S0140-6736(15)00308-6PubMedGoogle ScholarCrossref
20.
Shim SR, Kim SJ, Lee J, Rücker G. Network meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019013. doi:10.4178/epih.e2019013PubMedGoogle ScholarCrossref
21.
Shim SR, Kim SJ. Intervention meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019008. doi:10.4178/epih.e2019008PubMedGoogle ScholarCrossref
22.
Sachs GS, Yeung PP, Rekeda L, Khan A, Adams JL, Fava M. Adjunctive cariprazine for the treatment of patients with major depressive disorder: a randomized, double-blind, placebo-controlled phase 3 study. Am J Psychiatry. 2023;180(3):241-251. doi:10.1176/appi.ajp.20220504PubMedGoogle ScholarCrossref
23.
Riesenberg R, Yeung PP, Rekeda L, Sachs GS, Kerolous M, Fava M. Cariprazine for the adjunctive treatment of major depressive disorder in patients with inadequate response to antidepressant therapy: results of a randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2023;84(5):22m14643. doi:10.4088/JCP.22m14643PubMedGoogle ScholarCrossref
24.
Earley WR, Guo H, Németh G, Harsányi J, Thase ME. Cariprazine augmentation to antidepressant therapy in major depressive disorder: results of a randomized, double-blind, placebo-controlled trial. Psychopharmacol Bull. 2018;48(4):62-80. doi:10.64719/pb.4578PubMedGoogle ScholarCrossref
25.
Fava M, Durgam S, Earley W, et al. Efficacy of adjunctive low-dose cariprazine in major depressive disorder: a randomized, double-blind, placebo-controlled trial. Int Clin Psychopharmacol. 2018;33(6):312-321. doi:10.1097/YIC.0000000000000235PubMedGoogle ScholarCrossref
26.
Durgam S, Earley W, Guo H, et al. Efficacy and safety of adjunctive cariprazine in inadequate responders to antidepressants: a randomized, double-blind, placebo-controlled study in adult patients with major depressive disorder. J Clin Psychiatry. 2016;77(3):371-378. doi:10.4088/JCP.15m10070PubMedGoogle ScholarCrossref
27.
Kato M, Shiosakai M, Kuwahara K, et al. Adjunctive brexpiprazole 1 mg and 2 mg daily for Japanese patients with major depressive disorder following inadequate response to antidepressants: a phase 2/3, randomized, double-blind (BLESS) study. Psychiatry Clin Neurosci. 2024;78(2):113-122. doi:10.1111/pcn.13615PubMedGoogle ScholarCrossref
28.
Hobart M, Skuban A, Zhang P, et al. A randomized, placebo-controlled study of the efficacy and safety of fixed-dose brexpiprazole 2 mg/d as adjunctive treatment of adults with major depressive disorder. J Clin Psychiatry. 2018;79(4):17m12058. doi:10.4088/JCP.17m12058PubMedGoogle ScholarCrossref
29.
Hobart M, Skuban A, Zhang P, et al. Efficacy and safety of flexibly dosed brexpiprazole for the adjunctive treatment of major depressive disorder: a randomized, active-referenced, placebo-controlled study. Curr Med Res Opin. 2018;34(4):633-642. doi:10.1080/03007995.2018.1430220PubMedGoogle ScholarCrossref
30.
Thase ME, Youakim JM, Skuban A, et al. Adjunctive brexpiprazole 1 and 3 mg for patients with major depressive disorder following inadequate response to antidepressants: a phase 3, randomized, double-blind study. J Clin Psychiatry. 2015;76(9):1232-1240. doi:10.4088/JCP.14m09689PubMedGoogle ScholarCrossref
31.
Thase ME, Youakim JM, Skuban A, et al. Efficacy and safety of adjunctive brexpiprazole 2 mg in major depressive disorder: a phase 3, randomized, placebo-controlled study in patients with inadequate response to antidepressants. J Clin Psychiatry. 2015;76(9):1224-1231. doi:10.4088/JCP.14m09688PubMedGoogle ScholarCrossref
32.
Bauer M, Hefting N, Lindsten A, Josiassen MK, Hobart M. A randomised, placebo-controlled 24-week study evaluating adjunctive brexpiprazole in patients with major depressive disorder. Acta Neuropsychiatr. 2019;31(1):27-35. doi:10.1017/neu.2018.23PubMedGoogle ScholarCrossref
33.
Kamijima K, Kimura M, Kuwahara K, Kitayama Y, Tadori Y. Randomized, double-blind comparison of aripiprazole/sertraline combination and placebo/sertraline combination in patients with major depressive disorder. Psychiatry Clin Neurosci. 2018;72(8):591-601. doi:10.1111/pcn.12663PubMedGoogle ScholarCrossref
34.
Kamijima K, Higuchi T, Ishigooka J, et al; ADMIRE Study Group. Aripiprazole augmentation to antidepressant therapy in Japanese patients with major depressive disorder: a randomized, double-blind, placebo-controlled study (ADMIRE study). J Affect Disord. 2013;151(3):899-905. doi:10.1016/j.jad.2013.07.035PubMedGoogle ScholarCrossref
35.
Fava M, Mischoulon D, Iosifescu D, et al. A double-blind, placebo-controlled study of aripiprazole adjunctive to antidepressant therapy among depressed outpatients with inadequate response to prior antidepressant therapy (ADAPT-A study). Psychother Psychosom. 2012;81(2):87-97. doi:10.1159/000332050PubMedGoogle ScholarCrossref
36.
Berman RM, Fava M, Thase ME, et al. Aripiprazole augmentation in major depressive disorder: a double-blind, placebo-controlled study in patients with inadequate response to antidepressants. CNS Spectr. 2009;14(4):197-206. doi:10.1017/S1092852900020216PubMedGoogle ScholarCrossref
37.
Marcus RN, McQuade RD, Carson WH, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a second multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2008;28(2):156-165. doi:10.1097/JCP.0b013e31816774f9PubMedGoogle ScholarCrossref
38.
El-Khalili N, Joyce M, Atkinson S, et al. Extended-release quetiapine fumarate (quetiapine XR) as adjunctive therapy in major depressive disorder (MDD) in patients with an inadequate response to ongoing antidepressant treatment: a multicentre, randomized, double-blind, placebo-controlled study. Int J Neuropsychopharmacol. 2010;13(7):917-932. doi:10.1017/S1461145710000015PubMedGoogle ScholarCrossref
39.
Bauer M, Pretorius HW, Constant EL, Earley WR, Szamosi J, Brecher M. Extended-release quetiapine as adjunct to an antidepressant in patients with major depressive disorder: results of a randomized, placebo-controlled, double-blind study. J Clin Psychiatry. 2009;70(4):540-549. doi:10.4088/JCP.08m04629PubMedGoogle ScholarCrossref
40.
Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2007;68(6):843-853. doi:10.4088/JCP.v68n0604PubMedGoogle ScholarCrossref
41.
Durgam S, Earley WR, Kozauer SG, et al. Lumateperone as adjunctive therapy in patients with major depressive disorder: results from a randomized, double-blind, phase 3 trial. J Clin Psychiatry. 2025;86(4):25m15848. doi:10.4088/JCP.25m15848PubMedGoogle ScholarCrossref
42.
Durgam S, Earley WR, Kozauer SG, et al. Adjunctive lumateperone in patients with major depressive disorder: results from a randomized, double-blind, phase 3 trial. Am J Psychiatry. 2025;182(12):1072-1082. doi:10.1176/appi.ajp.20250292PubMedGoogle ScholarCrossref
43.
Duru G, Fantino B. The clinical relevance of changes in the Montgomery-Asberg Depression Rating Scale using the minimum clinically important difference approach. Curr Med Res Opin. 2008;24(5):1329-1335. doi:10.1185/030079908X291958PubMedGoogle ScholarCrossref
44.
Schalkwijk S, Undurraga J, Tondo L, Baldessarini RJ. Declining efficacy in controlled trials of antidepressants: effects of placebo dropout. Int J Neuropsychopharmacol. 2014;17(8):1343-1352. doi:10.1017/S1461145714000224PubMedGoogle ScholarCrossref
45.
Turkoz I, Alphs L, Singh J, et al. Clinically meaningful changes on depressive symptom measures and patient-reported outcomes in patients with treatment-resistant depression. Acta Psychiatr Scand. 2021;143(3):253-263. doi:10.1111/acps.13260PubMedGoogle ScholarCrossref
46.
Højlund M, Köhler-Forsberg O, Gregersen AT, et al. Prevalence, correlates, tolerability-related outcomes, and efficacy-related outcomes of antipsychotic polypharmacy: a systematic review and meta-analysis. Lancet Psychiatry. 2024;11(12):975-989. doi:10.1016/S2215-0366(24)00314-6PubMedGoogle ScholarCrossref
47.
Preskorn SH, Macaluso M, Trivedi M. How commonly used inclusion and exclusion criteria in antidepressant registration trials affect study enrollment. J Psychiatr Pract. 2015;21(4):267-274. doi:10.1097/PRA.0000000000000082PubMedGoogle ScholarCrossref
48.
Zimmerman M, Chelminski I, Posternak MA. Generalizability of antidepressant efficacy trials: differences between depressed psychiatric outpatients who would or would not qualify for an efficacy trial. Am J Psychiatry. 2005;162(7):1370-1372. doi:10.1176/appi.ajp.162.7.1370PubMedGoogle ScholarCrossref
49.
McIntyre RS, Sundararajan K, Behl S, et al. A double-blind, placebo-controlled, randomised withdrawal study of adjunctive brexpiprazole maintenance treatment for major depressive disorder. Acta Neuropsychiatr. 2024;37:e33. doi:10.1017/neu.2024.32PubMedGoogle ScholarCrossref
50.
McIntyre RS, Weiller E, Zhang P, Weiss C. Brexpiprazole as adjunctive treatment of major depressive disorder with anxious distress: results from a post-hoc analysis of two randomised controlled trials. J Affect Disord. 2016;201:116-123. doi:10.1016/j.jad.2016.05.013PubMedGoogle ScholarCrossref
51.
McIntyre RS, Bubolic S, Zhang Z, et al. Effects of adjunctive brexpiprazole on individual depressive symptoms and functioning in patients with major depressive disorder and anxious distress: post hoc analysis of three placebo-controlled studies. J Clin Psychopharmacol. 2024;44(2):133-140. doi:10.1097/JCP.0000000000001825PubMedGoogle ScholarCrossref
52.
Barabassy A, Csehi R, Dombi ZB, Szatmári B, Brevig T, Németh G. Transdiagnostic efficacy of cariprazine: a systematic review and meta-analysis of efficacy across ten symptom domains. Pharmaceuticals (Basel). 2025;18(7):995. doi:10.3390/ph18070995PubMedGoogle ScholarCrossref
53.
Fava M, Masand PS, Maletic V, Chen C, Adams JL, Kerolous M. Efficacy of adjunctive cariprazine on anxiety symptoms in patients with major depressive disorder: Post hoc analysis of a randomized placebo-controlled trial. J Clin Psychiatry. 2025;86(2):24m15506. doi:10.4088/JCP.24m15506PubMedGoogle ScholarCrossref
54.
Lee SH, Lee KH, Han TS, et al. The potential role of aripiprazole augmentation for major depressive disorder with anxious distress in naturalistic treatment setting. Clin Psychopharmacol Neurosci. 2024;22(2):370-375. doi:10.9758/cpn.23.1106PubMedGoogle ScholarCrossref
55.
Crapanzano C, Damiani S, Guiot C. Quetiapine in the anxiety dimension of mood disorders: a systematic review of the literature to support clinical practice. J Clin Psychopharmacol. 2021;41(4):436-449. doi:10.1097/JCP.0000000000001420PubMedGoogle ScholarCrossref
56.
McIntyre RS, Maletic V, Masand P, et al. The effect of adjunctive cariprazine on symptoms of anhedonia in patients with major depressive disorder. J Affect Disord. 2025;385(119366):119366. doi:10.1016/j.jad.2025.05.026PubMedGoogle ScholarCrossref
57.
McIntyre RS, Therrien F, Ismail Z, et al. Effects of adjunctive brexpiprazole on patient life engagement in major depressive disorder: post hoc analysis of Inventory of Depressive Symptomatology Self-Report data. J Psychiatr Res. 2023;162:71-78. doi:10.1016/j.jpsychires.2023.04.012PubMedGoogle ScholarCrossref
58.
Scheggi S, Pelliccia T, Gambarana C, De Montis MG. Aripiprazole relieves motivational anhedonia in rats. J Affect Disord. 2018;227:192-197. doi:10.1016/j.jad.2017.10.032PubMedGoogle ScholarCrossref
59.
Zisook S, Johnson GR, Tal I, et al. General predictors and moderators of depression remission: a VAST-D report. Am J Psychiatry. 2019;176(5):348-357. doi:10.1176/appi.ajp.2018.18091079PubMedGoogle ScholarCrossref
60.
McIntyre RS, Cha DS, Soczynska JK, et al. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depress Anxiety. 2013;30(6):515-527. doi:10.1002/da.22063PubMedGoogle ScholarCrossref
61.
Xiao N, Yin L, Lee S, et al. The efficacy of pharmacological interventions in the treatment of major depressive disorder and bipolar depression with mixed features: a systematic review. Bipolar Disord. 2025;27(5):347-357. doi:10.1111/bdi.70049PubMedGoogle ScholarCrossref
62.
Teopiz KM, Lo HKY, Lakhani M, et al. Should glutamatergic modulators be considered preferential treatments for adults with major depressive disorder and a reported history of trauma? conceptual and clinical implications. CNS Spectr. 2025;30(1):e61. doi:10.1017/S1092852925100278PubMedGoogle ScholarCrossref
63.
McIntyre RS. Acetylcholine and muscarinic receptor targeting in bipolar disorder: does xanomeline-trospium chloride and other investigational muscarinic agonists hold promise as mechanistically informed treatments for manic episodes, mixed features and cognitive deficits in bipolar disorder? Expert Opin Investig Drugs. 2025;34(6):519-526. doi:10.1080/13543784.2025.2522885PubMedGoogle ScholarCrossref
64.
Jain R, Maletic V, McIntyre RS. Diagnosing and treating patients with mixed features. J Clin Psychiatry. 2017;78(8):1091-1102. doi:10.4088/JCP.su17009ah1cPubMedGoogle ScholarCrossref
65.
Suppes T, Silva R, Cucchiaro J, et al. Lurasidone for the treatment of major depressive disorder with mixed features: a randomized, double-blind, placebo-controlled study. Am J Psychiatry. 2016;173(4):400-407. doi:10.1176/appi.ajp.2015.15060770PubMedGoogle ScholarCrossref
66.
McIntyre RS, Llorca PM, Aronin LC, Yu J, Nguyen HB. Effect of cariprazine on anhedonia in patients with bipolar I depression: post hoc analysis of three randomized placebo-controlled clinical trials. Adv Ther. 2025;42(1):246-260. doi:10.1007/s12325-024-03009-2PubMedGoogle ScholarCrossref
67.
Jain R, McIntyre RS, Cutler AJ, et al. Efficacy of cariprazine in patients with bipolar depression and higher or lower levels of baseline anxiety: a pooled post hoc analysis. Int Clin Psychopharmacol. 2024;39(2):82-92. doi:10.1097/YIC.0000000000000500PubMedGoogle ScholarCrossref
68.
Trivedi MH, Thase ME, Fava M, et al. Adjunctive aripiprazole in major depressive disorder: analysis of efficacy and safety in patients with anxious and atypical features. J Clin Psychiatry. 2008;69(12):1928-1936. doi:10.4088/JCP.v69n1211PubMedGoogle ScholarCrossref
69.
Thase ME, Demyttenaere K, Earley WR, Gustafsson U, Udd M, Eriksson H. Extended release quetiapine fumarate in major depressive disorder: analysis in patients with anxious depression. Depress Anxiety. 2012;29(7):574-586. doi:10.1002/da.21970PubMedGoogle ScholarCrossref
70.
McIntyre RS, Rosenblat JD, Nemeroff CB, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: an international expert opinion on the available evidence and implementation. Am J Psychiatry. 2021;178(5):383-399. doi:10.1176/appi.ajp.2020.20081251PubMedGoogle ScholarCrossref
71.
Akbar D, Rhee TG, Ceban F, et al. Dextromethorphan-bupropion for the treatment of depression: a systematic review of efficacy and safety in clinical trials. CNS Drugs. 2023;37(10):867-881. doi:10.1007/s40263-023-01032-5PubMedGoogle ScholarCrossref
72.
Lenze EJ; OPTIMUM Study Group. Antidepressant augmentation versus switch in treatment-resistant geriatric depression. reply. N Engl J Med. 2023;388(21):2013. doi:10.1056/NEJMoa2204462PubMedGoogle ScholarCrossref
73.
Mohamed S, Johnson GR, Chen P, et al; and the VAST-D Investigators. Effect of antidepressant switching vs augmentation on remission among patients with major depressive disorder unresponsive to antidepressant treatment: the VAST-D randomized clinical trial. JAMA. 2017;318(2):132-145. doi:10.1001/jama.2017.8036
ArticlePubMedGoogle ScholarCrossref
74.
Papakostas GI, Trivedi MH, Shelton RC, et al. Comparative effectiveness research trial for antidepressant incomplete and non-responders with treatment resistant depression (ASCERTAIN-TRD) a randomized clinical trial. Mol Psychiatry. 2024;29(8):2287-2295. doi:10.1038/s41380-024-02468-xPubMedGoogle ScholarCrossref
75.
Ji M, Feng J, Liu G. Efficacy and safety of aripiprazole or bupropion augmentation and switching in patients with treatment-resistant depression or major depressive disorder: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2024;19(4):e0299020. doi:10.1371/journal.pone.0299020PubMedGoogle ScholarCrossref
76.
Vieta E, Ahmed N, Arango C, et al. Improvements in functioning and workplace productivity with esketamine nasal spray versus quetiapine extended release in patients with treatment resistant depression: findings from a 32-week randomised, open-label, rater-blinded phase IIIb study. Eur Neuropsychopharmacol. 2025;93:29-39. doi:10.1016/j.euroneuro.2024.12.013PubMedGoogle ScholarCrossref
77.
McIntyre RS, Mattingly G, Godinov Y, et al. Esketamine nasal spray versus quetiapine XR in adults with treatment-resistant depression: a secondary analysis of the ESCAPE-TRD randomized clinical trial. CNS Spectr. 2025;30(1):e26. doi:10.1017/S1092852924002451PubMedGoogle ScholarCrossref
78.
McIntyre RS, Bitter I, Buyze J, et al. Safety and tolerability of esketamine nasal spray versus quetiapine extended release in patients with treatment resistant depression. Eur Neuropsychopharmacol. 2024;85:58-65. doi:10.1016/j.euroneuro.2024.05.009PubMedGoogle ScholarCrossref
79.
Reif A, Bitter I, Buyze J, et al; ESCAPE-TRD Investigators. Esketamine nasal spray versus quetiapine for treatment-resistant depression. N Engl J Med. 2023;389(14):1298-1309. doi:10.1056/NEJMoa2304145PubMedGoogle ScholarCrossref
80.
Calder CN, Kwan ATH, Teopiz KM, et al. Number needed to treat (NNT) for ketamine and esketamine in adults with treatment-resistant depression: a systematic review and meta-analysis. J Affect Disord. 2024;356:753-762. doi:10.1016/j.jad.2024.04.039PubMedGoogle ScholarCrossref
81.
Liebowitz M, Lam RW, Lepola U, Datto C, Sweitzer D, Eriksson H. Efficacy and tolerability of extended release quetiapine fumarate monotherapy as maintenance treatment of major depressive disorder: a randomized, placebo-controlled trial. Depress Anxiety. 2010;27(10):964-976. doi:10.1002/da.20740PubMedGoogle ScholarCrossref
82.
Fugger G, Bartova L, Dold M, et al. Evidence on sociodemographic and clinical correlates of antidepressant combination or augmentation with second-generation antipsychotics in major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2022;114(110480):110480. doi:10.1016/j.pnpbp.2021.110480PubMedGoogle ScholarCrossref